
Effects of Vitamin D in Post-Exercise Muscle Recovery. A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Searching Strategies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Potential Bias Risk
2.5. Statistical Analysis
3. Results
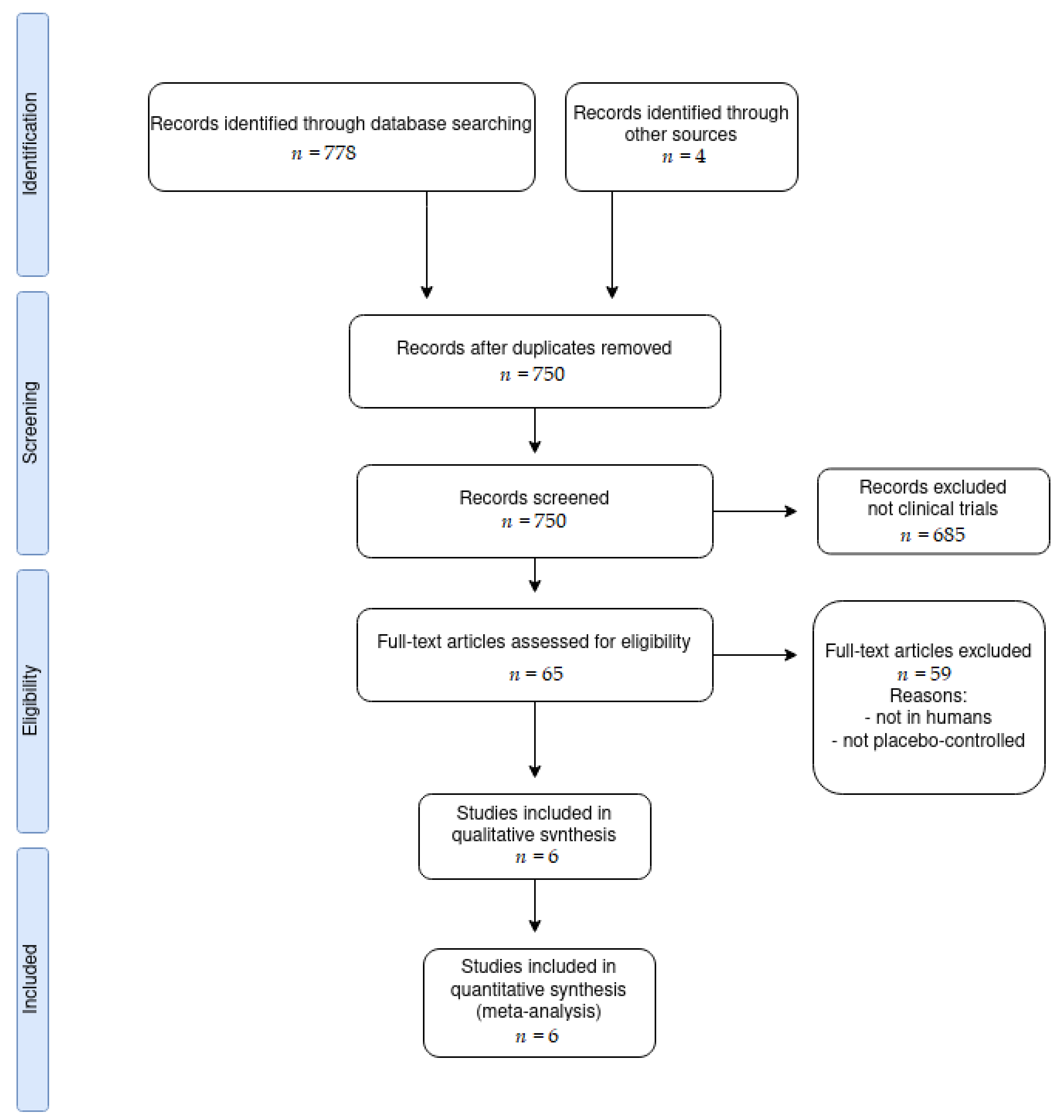
3.1. Article Search
3.2. Vitamin D Administration Protocols
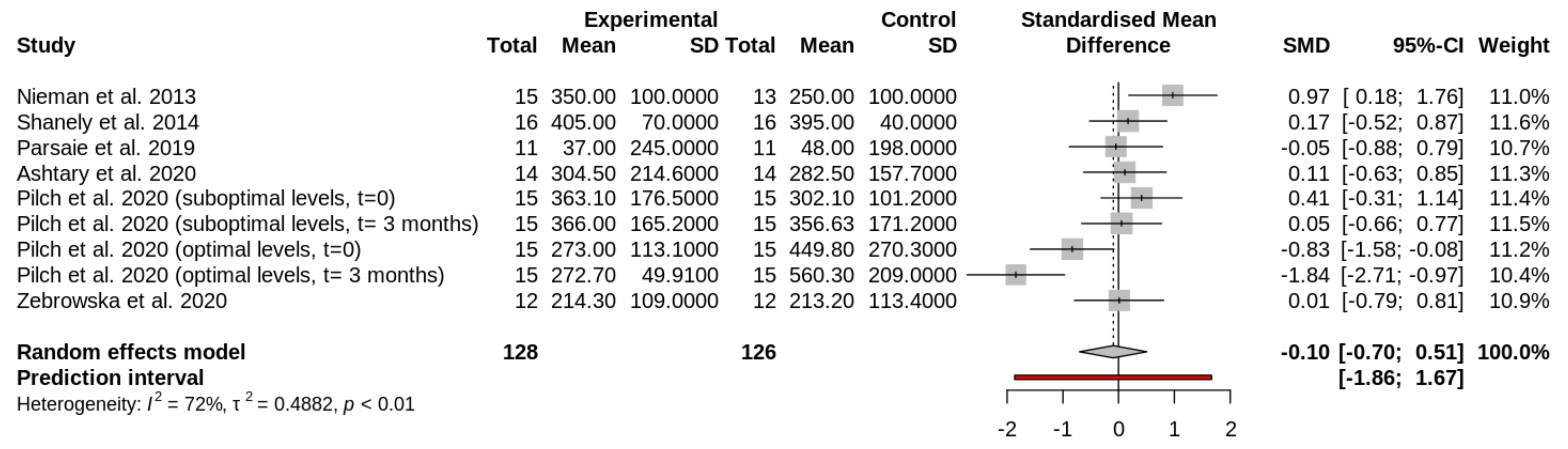
3.3. Effect of Vitamin D Supplementation on Circulating Creatine Kinase Levels
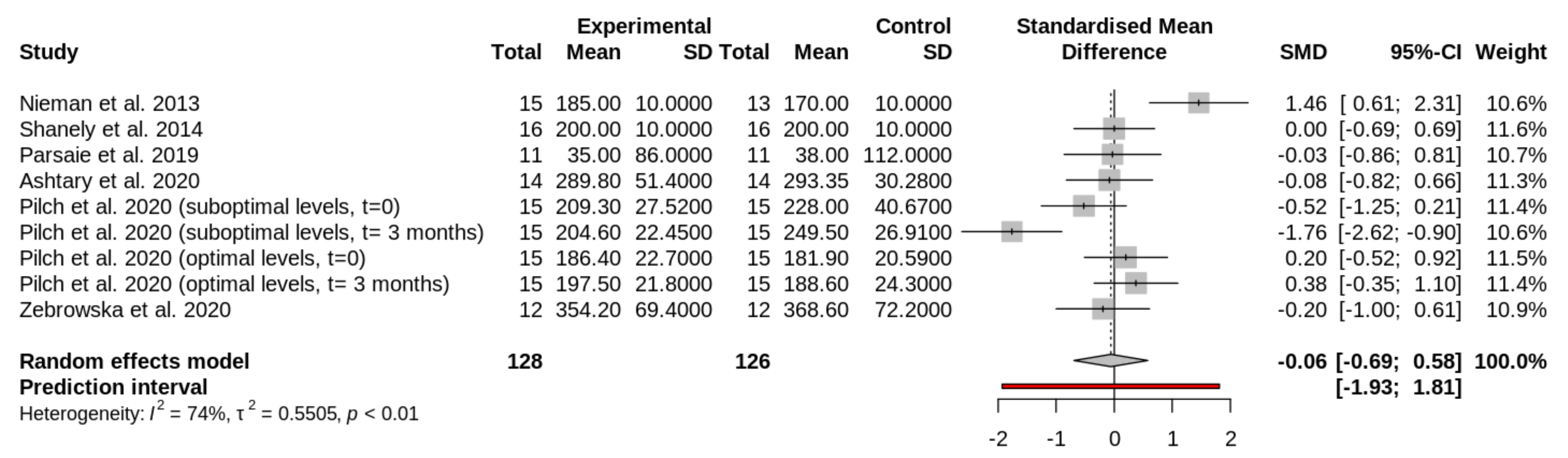
3.4. Effect of Vitamin D Supplementation on Circulating Lactate Dehydrogenase Levels
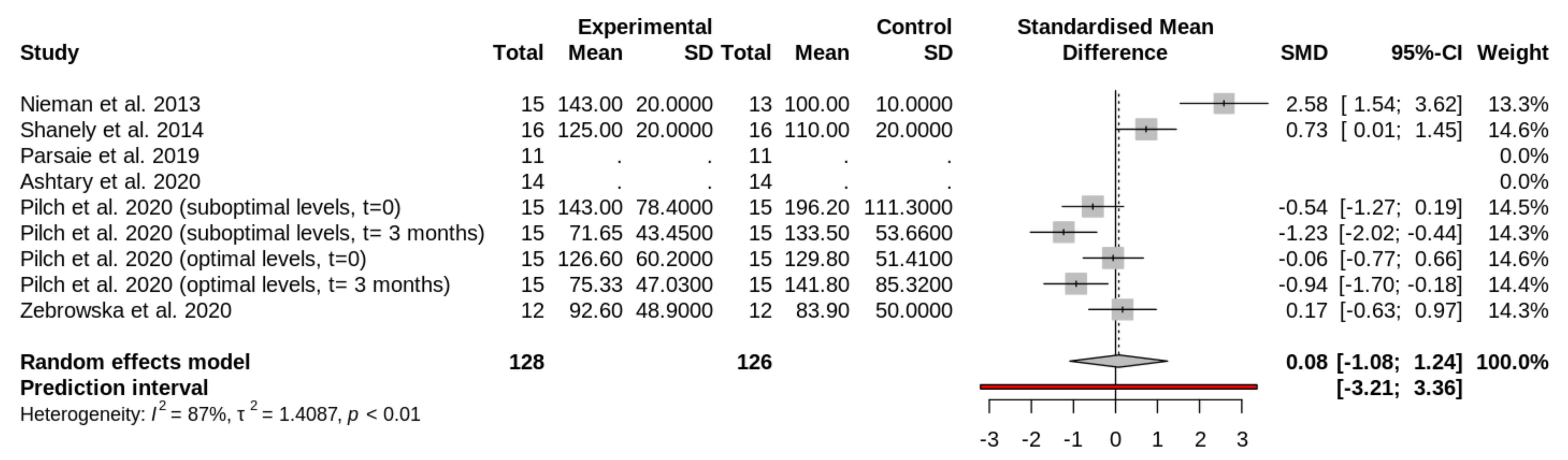
3.5. Effect of Vitamin D Supplementation on Circulating Myoglobin Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. Vitamin D and innate and adaptive immunity. In Vitamins & Hormones; Litwack, G., Ed.; Elsevier: Barcelona, Spain, 2011; Volume 86, pp. 23–62. [Google Scholar]
- Xu, H.; Soruri, A.; Gieseler, R.K.; Peters, J.H. 1,25-Dihydroxyvitamin D3 exerts opposing effects to IL-4 on MHC class-II antigen expression, accessory activity, and phagocytosis of human monocytes. Scand. J. Immunol. 1993, 38, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Larsen-Meyer, D.E.; Willis, K.S. Vitamin D and athletes. Curr. Sports Med. Rep. 2010, 9, 220–226. [Google Scholar] [CrossRef]
- Willis, K.S.; Smith, D.T.; Broughton, K.S.; Larson-Meyer, D.E. Vitamin D status and biomarkers of inflammation in runners. J. Sports Med. 2012, 3, 35–42. [Google Scholar]
- Campbell, P.M.F.; Allain, T.J. Muscle strength and vitamin D in older people. Gerontology 2006, 52, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Ceglia, L. Vitamin D and skeletal muscle tissue and function. Mol. Asp. Med. 2008, 29, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Ceglia, L.; Harris, S.S. Vitamin D and its role in skeletal muscle. Calcif. Tissue Int. 2013, 92, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Irani, P.F. Electromyography in nutritional osteomalacic myopathy. J. Neurol. Neurosurg. Psychiatry 1976, 10, 686–693. [Google Scholar] [CrossRef][Green Version]
- Barker, T.; Henriksen, V.T.; Martins, T.B.; Hill, H.R.; Kjeldsberg, C.R.; Schneider, E.D.; Dixon, B.M.; Weaver, L.K. Higher serum 25-hydroxyvitamin D concentrations associate with a faster recovery of skeletal mscle strength after muscular injury. Nutrients 2013, 5, 1253–1275. [Google Scholar] [CrossRef]
- Stratos, I.; Li, Z.; Herlyn, P.; Rotter, R.; Behrendt, A.K.; Mittlmeier, T.; Vollmar, B. Vitamin D increases cellular turnover and functionally restores the skeletal muscle after crush injury in rats. Am. J. Pathol. 2013, 182, 895–904. [Google Scholar] [CrossRef]
- Paulsen, G.; Mikkelsen, U.R.; Raastad, T.; Peake, J.M. Leucocytes, cytokines and satellite cells: What role do they play in muscle damage and regeneration following eccentric exercise? Exerc. Immunol. Rev. 2012, 18, 42–97. [Google Scholar] [PubMed]
- Khan, F.Y. Rhabdomyolysis: A review of the literature. Neth. J. Med. 2009, 67, 272–283. [Google Scholar]
- Brancaccio, P.; Maffulli, N.; Limongelli, F.M. Creatine kinase monitoring in sport medicine. Br. Med. Bull. 2007, 81–82, 209–230. [Google Scholar] [CrossRef] [PubMed]
- Bessa, A.; Oliveira, V.N.; De Agostini, G.G.; Oliveira, R.J.; Oliveira, A.C.; White, G.; Wells, G.; Teixeira, D.N.; Espindola, F.S. Exercise intensity and recovery: Biomarkers of injury, inflammation and oxidative stress. J. Strength Cond. Res. 2013, 30, 311–319. [Google Scholar] [CrossRef]
- Brancaccio, P.; Maffulli, N.; Buonauro, R.; Limongelli, F.M. Serum enzyme monitoring in sports medicine. Clin. Sports Med. 2008, 27, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Clarkson, P.M. Plasma creatine kinase activity and glutathione after eccentric exercise. Med. Sci. Sports Exerc. 2003, 35, 930–936. [Google Scholar] [CrossRef]
- Banfi, G.; Colombini, A.; Lombardi, G.; Lubkowska, A. Metabolic markers in Sports Medicine. Adv. Clin. Chem. 2012, 56, 1–54. [Google Scholar]
- Baird, M.F.; Graham, S.M.; Baker, J.S.; Bickerstaff, G.F. Creatine-kinase- and exercise-related muscle damage implications for muscle performance and recovery. J. Nutr. Metab. 2012, 2012, 1–13. [Google Scholar] [CrossRef]
- Vincent, H.K.; Vincent, K.R. The effect of training status on the serum creatine kinase response, soreness and muscle function following resistance exercise. Int. J. Sports Med. 1997, 18, 431–437. [Google Scholar] [CrossRef]
- Horská, A.; Fishbein, K.W.; Fleg, J.L.; Spencer, R.G. The relationship between creatine kinase kinetics and exercise intensity in human forearm is unchanged by age. Am. J. Physiol. Endocrinol. Metab. 2000, 279, 333–339. [Google Scholar] [CrossRef]
- Hackney, A.C.; Walz, E.A. Hormonal adaptation and the stress of exercise training: The role of glucocorticoids. Trends Sport Sci. 2013, 20, 165–171. [Google Scholar]
- Martinez, A.C.; Seco-Calvo, J.; Tur-Mari, J.A.; Abecia-Inchaurregui, L.C.; Orella, E.E.; Pons-Biescas, A. Testosterone and cortisol changes in professional basketball players through a season competition. J. Strength Cond. Res. 2010, 24, 1102–1108. [Google Scholar] [CrossRef]
- Cordova, A.; Martin, J.F.; Reyes, E.; Alvarez-Mon, M. Protection against muscle damage in competitive sports players: The effect of the mmunomodulator AM3. J. Sports Sci. 2004, 22, 827–833. [Google Scholar] [CrossRef]
- Cordova, A.; Mielgo-Ayuso, J.; Fernandez-Lazaro, C.I.; Caballero-García, A.; Roche, E.; Fernández-Lázaro, D. Effect of iron supplementation on the modulation of iron metabolism, muscle damage biomarkers and cortisol in professional cyclists. Nutrients 2019, 11, 500. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Buckinx, F.; Rabenda, V.; Gillain, S.; Cavalier, E.; Slomian, J.; Bruyere, O. The effects of vitamin D on skeletal muscle strength, muscle mass, and muscle power: A systematic review and meta-analysis of randomized controlled trials. J. Clin. Endocrinol. Metab. 2014, 99, 4336–4345. [Google Scholar] [CrossRef] [PubMed]
- Salminen, M.; Saaristo, P.; Salonoja, M.; Vaapio, S.; Vahlberg, T.; Lamberg-Allardt, C.; Kivela, S.L. Vitamin D status and physical function in older Finnish people: A one-year follow-up study. Arch. Gerontol. Geriatr. 2015, 61, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Park, H.; Cho, S.; Lee, M. Vitamin D3 supplementation modulates inflammatory responses from the muscle damage induced by high-intensity exercise in SD rats. Cytokine 2013, 63, 27–35. [Google Scholar] [CrossRef]
- Tomlinson, P.B.; Joseph, C.; Angioi, M. Effects of vitamin D supplementation on upper and lower body muscle strength levels in healthy individuals. A systematic review with meta-analysis. J. Sci. Med. Sport 2015, 18, 575–580. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- O’Connor, D.; Green, S.; Higgins, J.P.T. Defining the review question and developing criteria for including studies. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Green, S., Eds.; John Wiley & Sons, Ltd.: Chichester, UK, 2008; pp. 81–94. [Google Scholar]
- Nieman, D.C.; Gillitt, N.D.; Shanely, R.A.; Dew, D.; Meaney, M.P.; Luo, B. Vitamin D2 supplementation amplifies eccentric exercise-induced muscle damage in NASCAR Pit Crew athletes. Nutrients 2013, 6, 63–75. [Google Scholar] [CrossRef]
- Shanely, R.A.; Nieman, D.C.; Knab, A.M.; Gillitt, N.D.; Meaney, M.P.; Jin, F.; Sha, W.; Cialdella-Kam, L. Influence of vitamin D mushroom powder supplementation on exercise-induced muscle damage in vitamin D insufficient high school athletes. J. Sports Sci. 2014, 32, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Parsaie, N.; Ghavamzadeh, S.; Cheraghi, M. Effects of cholecalciferol supplementation on inflammatory markers and muscle damage indices of soccer players after a simulated soccer match. Nutrition 2019, 59, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Ashtary-Larky, D.; Kheirollah, A.; Bagheri, R.; Ghaffari, M.A.; Mard, S.A.; Hashemi, S.J.; Mir, I.; Wong, A. A single injection of vitamin D3 improves insulin sensitivity and β-cell function but not muscle damage or the inflammatory and cardiovascular responses to an acute bout of resistance exercise in vitamin D-deficient resistance-trained males. Br. J. Nutr. 2020, 123, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Pilch, W.; Kita, B.; Piotrowska, A.; Tota, L.; Maciejczyk, M.; Czerwińska-Ledwig, O.; Sadowska-Krepa, E.; Kita, S.; Pałka, T. The effect of vitamin D supplementation on the muscle damage after eccentric exercise in young men: A randomized, control trial. J. Int. Soc. Sports Nutr. 2020, 17, 53. [Google Scholar] [CrossRef]
- Żebrowska, A.; Sadowska-Krępa, E.; Stanula, A.; Waśkiewicz, Z.; Łakomy, O.; Bezuglov, E.; Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. The effect of vitamin D supplementation on serum total 25(OH) levels and biochemical markers of skeletal muscles in runners. J. Int. Soc. Sports Nutr. 2020, 17, 18. [Google Scholar] [CrossRef]
- Hedges, L.V. Distribution theory for glass’s estimator of effect size and related estimators. J. Educ. Behav. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley Cochrane Series: Hoboken, NJ, USA, 2019. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Russell, J.; Cobley, J.N.; Owens, D.J.; Wilson, G.; Gregson, W.; Morton, J.P. Assessment of vitamin D concentration in non-supplemented professional athletes and healthy adults during the winter months in the UK: Implications for skeletal muscle function. J. Sports Sci. 2013, 31, 344–353. [Google Scholar] [CrossRef]
- Owens, D.J.; Webber, D.; Impey, S.G.; Tang, J.; Donovan, T.F.; Fraser, W.D.; Close, G.L. Vitamin D supplementation does not improve human skeletal muscle contractile properties in insufficient young males. Eur. J. Appl. Physiol. 2014, 114, 1309–1320. [Google Scholar] [CrossRef]
- Owens, D.J.; Sharples, A.P.; Polydorou, I.; Alwan, N.; Donovan, T.; Tang, J.; Close, G.L. A systems-based investigation into vitamin D and skeletal muscle repair, regeneration, and hypertrophy. Am. J. Physiol. Endocrinol. Metab. 2015, 309, E1019–E1031. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.M.; Redzic, M.; Thomas, D.T. The effects of season-long vitamin D supplementation on collegiate swimmers and divers. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.; Schneider, E.D.; Dixon, B.M.; Henriksen, V.T.; Weaver, L.K. Supplemental vitamin D enhances the recovery in peak isometric force shortly after intense exercise. Nutr. Metab. 2013, 10, 69. [Google Scholar] [CrossRef]
- Clarkson, P.M.; Hubal, M.J. Exercise-induced muscle damage in humans. Am. J. Phys. Med. Rehabil. 2002, 81, 52–69. [Google Scholar] [CrossRef] [PubMed]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hypponen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef]
- Caballero-García, A.; Córdova-Martínez, A.; Vicente-Salar, N.; Roche, E.; Pérez-Valdecantos, D. Vitamin D, Its role in recovery after muscular damage following exercise. Nutrients 2021, 13, 2336. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Randomized (Selection Bias) | Blinding of Participants (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) |
|---|---|---|---|
| Nieman et al., 2013 [32] | + | + | + |
| Shanely et al., 2014 [33] | + | + | + |
| Parsaie et al., 2019 [34] | + | + | + |
| Ashtary-Larky et al., 2020 [35] | + | + | + |
| Pilch et al., 2020 [36] | + | − | − |
| Żebrowska et al., 2020 [37] | − | + | + |
| Athletic level of participants | Young men/High school | 2 studies: Pilch et al., 2020 [36] Shanely et al., 2014 [33] |
| Resistance-trained men/Male runners | 2 studies: Ashtary-Larky et al., 2020 [35] Żebrowska et al., 2020 [37] | |
| Male soccer players | 1 study: Parsaie et al., 2019 [34] | |
| NASCAR pit crew | 1 study: Nieman et al., 2013 [32] | |
| Age of participants | <20 years old | 1 study: Shanely et al., 2014 [33] |
| 20–30 years old | 4 studies: Nieman et al., 2013 [32] Parsaie et al., 2019 [34] Ashtary-Larky et al., 2020 [35] Pilch et al., 2020 [36] | |
| 30–40 years old | 1 study: Żebrowska et al., 2020 [37] | |
| Vitamin D administration | Ingestion | 5 studies: Nieman et al., 2013 [32] Parsaie et al., 2019 [34] Pilch et al., 2020 [36] Shanely et al., 2014 [33] Żebrowska et al., 2020 [37] |
| Injection | 1 study: Ashtary-Larky et al., 2020 [35] | |
| Vitamin D dose (type) | 600 IU/day (vitD2) | 1 study: Shanely et al., 2014 [33] |
| 2000 IU/week (vitD3) | 1 study: Żebrowska et al., 2020 [37] | |
| 3800 IU/day (vitD2) | 1 study: Nieman et al., 2013 [32] | |
| 50,000 IU/day (vitD3) | 1 study: Parsaie et al., 2019 [34] | |
| 300,000 IU injected in one dose (vitD3) | 1 study: Ashtary-Larky et al., 2020 [35] | |
| Calculated from participant’s body mass using Singh and Bonham formula (vitD3) | 1 study: Pilch et al., 2020 [36] | |
| Extent of supplementation | 3 weeks | 1 study: Żebrowska et al., 2020 [37] |
| 4 weeks | 1 study: Ashtary-Larky et al., 2020 [35] | |
| 6 weeks | 2 studies: Nieman et al., 2013 [32] Shanely et al., 2014 [33] | |
| 8 weeks | 1 study: Parsaie et al., 2019 [34] | |
| 12 weeks | 1 study: Pilch et al., 2020 [36] | |
| Exercise type | Eccentric exercise | 3 studies: Nieman et al., 2013 [32] Pilch et al., 2020 [36] Żebrowska et al., 2020 [37] |
| Loughborough intermittent shuttle test | 2 studies: Parsaie et al., 2019 [34] Shanely et al., 2014 [33] | |
| Acute resistance exercise (different presses and weights) | 1 study: Ashtary-Larky et al., 2020 [35] |
| Study | Circulating Vitamin D Levels (ng/mL) before the Study | Dose (IU) | Extent |
|---|---|---|---|
| Nieman et al., 2013 [32] | 39 ± 2 (Experimental group *) 43 ± 3 (Placebo group) | 3800 IU/day | 6 weeks |
| Shanely et al., 2014 [33] | 25 ± 2 (Experimental group *) 25 ± 2 (Placebo group) | 600 IU/day | 6 weeks |
| Parsaie et al., 2019 [34] | 14 (Experimental group *) 15 (Placebo group) | 50,000 IU/week | 8 weeks |
| Ashtary-Larky et al., 2020 [35] | 14 ± 3.9 (Experimental group *) 22 ± 5 (Placebo group) | 300,000 IU injected | 4 weeks |
| Pilch et al., 2020 [36] | 30.5 ± 0.34 (OE group: Optimal levels of vitamin D at the beginning and supplemented during the intervention) 36.16 ± 4.4 (OC group: Optimal levels of vitamin D at the beginning and no supplemented during the intervention) 19 ± 1 (SE group: Suboptimal levels of vitamin D at the beginning and supplemented during the intervention) 14 ± 5 (SC group: Suboptimal levels of vitamin D at the beginning and no supplemented during the intervencion) | Calculated from participant’s body mass using Singh and Bonham formula. | 12 weeks |
| Żebrowska et al., 2020 [37] | 40 ± 8.8 (Experimental group *) 33.3 ± 3.4 (Placebo group) | 2000 IU/day | 3 weeks |
| Study | Sample Size | Analyzed Parameters (Time for Measurement) | Main Outcomes |
|---|---|---|---|
| Nieman et al., 2013 [32] | 28 | CK, LDH, Mb (immediately after exercise execution) | ↑CK, ↑LDH, ↑Mb |
| Shanely et al., 2014 [33] | 50 | CK, LDH, Mb (immediately after exercise execution) | =CK, =LDH, =Mb |
| Parsaie et al., 2019 [34] | 22 | CK, LDH (immediately after exercise execution) | =CK, =LDH |
| Ashtary-Larky et al., 2020 [35] | 14 | CK, LDH (1 h after exercise execution) | =CK, =LDH |
| Pilch et al., 2020 [36] | 60 | CK, LDH, Mb (1 h after exercise execution) | ↓CK, ↓LDH, ↓Mb * |
| Żebrowska et al., 2020 [37] | 24 | CK, LDH, Mb (1 h after exercise execution) | ↓CK, ↓LDH, ↓Mb |
| Study | Limitations |
|---|---|
| Nieman et al., 2013 [32] | Physical activity consists in a very specific job, difficult to compare with other sport disciplines. Small sample size. Gender not specified (likely men). Supplementation with ergocalciferol. |
| Shanely et al., 2014 [33] | Information regarding the physical activity performed is limited, being complicated the comparison with other studies. Analytical method for vitamin D determination: chemiluminescent immunoassay. Performed only in men. Supplementation with ergocalciferol. |
| Parsaie et al., 2019 [34] | Analytical method for vitamin D determination: immunoassay. Small sample size. Gender not specified. Differences in baseline BMI between groups. |
| Ashtary-Larky et al., 2020 [35] | The exact type of endurance activity is not indicated. Analytical method for vitamin D determination: immunoassay (ELISA). Small sample size. Performed only in men. Short duration.One dose of vitamin D. |
| Pilch et al., 2020 [36] | Subjective control of the physical activity performed. The intensity is difficault to compare with other studies. Analytical method for vitamin D determination: immunoassay (ELISA). Performed only in men. |
| Żebrowska et al., 2020 [37] | Analytical method for vitamin D determination: no indicated. Small sample size. Performed only in men. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bello, H.J.; Caballero-García, A.; Pérez-Valdecantos, D.; Roche, E.; Noriega, D.C.; Córdova-Martínez, A. Effects of Vitamin D in Post-Exercise Muscle Recovery. A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 4013. https://doi.org/10.3390/nu13114013
Bello HJ, Caballero-García A, Pérez-Valdecantos D, Roche E, Noriega DC, Córdova-Martínez A. Effects of Vitamin D in Post-Exercise Muscle Recovery. A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(11):4013. https://doi.org/10.3390/nu13114013
Chicago/Turabian StyleBello, Hugo J., Alberto Caballero-García, Daniel Pérez-Valdecantos, Enrique Roche, David C. Noriega, and Alfredo Córdova-Martínez. 2021. "Effects of Vitamin D in Post-Exercise Muscle Recovery. A Systematic Review and Meta-Analysis" Nutrients 13, no. 11: 4013. https://doi.org/10.3390/nu13114013
APA StyleBello, H. J., Caballero-García, A., Pérez-Valdecantos, D., Roche, E., Noriega, D. C., & Córdova-Martínez, A. (2021). Effects of Vitamin D in Post-Exercise Muscle Recovery. A Systematic Review and Meta-Analysis. Nutrients, 13(11), 4013. https://doi.org/10.3390/nu13114013